 Download biomedica product list 2018
Download biomedica product list 2018Big Endothelin-1 ELISA



-
Category number
BI-20082H
-
Method
Sandwich ELISA, HRP/TMB, 12×8-well detachable strips
-
Sample type
Serum, EDTA plasma, citrate plasma, heparin plasma
-
Sample volume
50 µl / well
-
Assay time
4 h / 1 h / 30 min
-
Sensitivity
0.02 pmol/l (= 0.086 pg/ml)
-
Standard range
0 – 3 pmol/l (= 0 – 12.85 pg/ml)
-
Conversion factor
1 pg/ml = 0.2335 pmol/l (MW: 4.283 kDa)
-
Specificity
Endogenous and recombinant Big Endothelin-1 (Big ET-1).
-
Precision
In-between-run (n=5): ≤ 4 % CV
Within-run (n=5): ≤ 5 % CV
-
Cross-reactivity
Human ET1/2/3 (1-21): <1%, human ET2 (1-37): <1%, human ET1/2 (1-38): <1%, human BigET1/2 (22-38) : <1%, human BigET2 (22-37) : <1%,
porcine BigET (1-39): 21%, rat BigET1 (1-39): 10%, Sarafotoxin: <1%
-
Use
CE marked – for IVD use in the EU
-
Validation Data
See validation data tab for: precision, accuracy, diltuion linearity, values for healthy donors, etc.
Product Overview
The Big Endothelin-1 immunoassay is a 5.5 hour, 96-well sandwich ELISA for the quantitative determination of Big Endothelin-1 in serum and plasma. The assay employs human serum-based standards to ensure the measurement of biologically reliable data.
Principle of the Assay
The Big Endothelin-1 ELISA kit is a sandwich enzyme immunoassay for the quantitative determination of Big Endothelin-1 in human serum and plasma samples.
The figure below explains the principle of the Big Endothelin-1 sandwich ELISA:
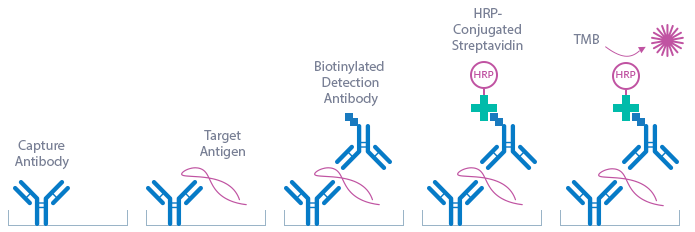
In a first step, standard/control/sample and detection antibody (monoclonal mouse anti- human Big Endothelin-1 antibody) are pipetted into the wells of the microtiter strips, which are pre-coated with polyclonal sheep anti-human Big Endothelin-1 antibody. Big Endothelin-1 present in the standard/control/sample binds to the pre-coated antibody in the well and forms a sandwich with the detection antibody. After a washing step, which removes all non-specifically bound and unbound material, the conjugate (streptavidin-HRP) is pipetted into the wells and reacts with the detection antibody. After another washing step, the substrate (tetramethylbenzidine, TMB) is pipetted into the wells. The enzyme-catalyzed color change of the substrate is directly proportional to the amount of Big Endothelin-1. This color change is detectable with a standard microtiter plate reader. The concentration of Big Endothelin-1 in the sample is determined directly from the dose response curve.
The antibodies utilized in the Big Endothelin-1 ELISA (BI-20082H) are as follows:
Capture Antibody: polyclonal sheep-anti human Big Endothelin-1
Detection Antibody: monoclonal mouse anti-human Big Endothelin-1
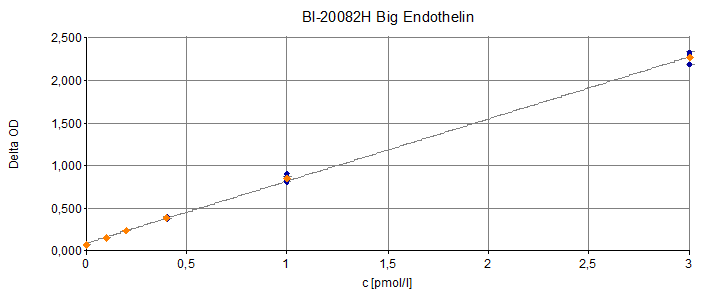
Typical Standard Curve
The figure below shows a typical standard curve for the Big Endothelin-1 ELISA. The immunoassay is calibrated against recombinant Big Endothelin-1 peptide:
ELISA Kit Components
|
Contents |
Description |
Quantity |
|
PLATE |
Polyclonal sheep anti-human Big Endothelin-1 antibody pre-coated microtiter strips in strip holder, packed in aluminum bag with desiccant |
12 x 8 tests |
|
WASHBUF |
Wash buffer concentrate 20x, natural cap |
1 x 50 ml |
|
STD |
Standards 1-6, (0; 0.10; 0.20; 0.40; 1; 3 pmol/l), synthetic human Big Endothelin-1 in human serum, white caps, lyophilized |
6 vials |
|
CTRL |
Control, yellow cap, lyophilized, exact concentration see label |
1 vial |
|
AB |
Monoclonal mouse anti-human Big Endothelin-1 antibody, biotin labeled, red dye, green cap, ready to use |
1 x 18 ml |
|
CONJ |
Conjugate, (streptavidin-HRP), amber cap, ready to use |
1 x 22 ml |
|
SUB |
Substrate, (TMB solution), blue cap, ready to use |
1 x 22 ml |
|
STOP |
Stop solution, white cap, ready to use |
1 x 7 ml |
Storage instructions: All reagents of the Big Endothelin-1 ELISA kit are stable at 4°C until the expiry date stated on the label of each reagent.
Serum, EDTA plasma, heparin plasma, citrate plasma, cell culture supernatant and urine are suitable for use in this assay. Do not change sample type during studies. We recommend duplicate measurements for all samples, standards and controls. The sample collection and storage conditions listed are intended as general guidelines.
Serum & Plasma
Collect venous blood samples in standardized serum separator tubes (SST) or standardized blood collection tubes using EDTA, heparin or citrate as an anticoagulant. For serum samples, allow samples to clot for 30 minutes at room temperature. Perform separation by centrifugation according to the tube manufacturer’s instructions for use. Assay the acquired samples immediately or aliquot and store at -25°C or lower. Lipemic or haemolyzed samples may give erroneous results. Do not freeze-thaw samples more than four times.
Reagent Preparation
Wash Buffer
|
1. |
Bring the WASHBUF concentrate to room temperature. Crystals in the buffer concentrate will dissolve at room temperature (18-26°C). |
|
2. |
Dilute the WASHBUF concentrate 1:20, e.g. 50 ml WASHBUF + 950 ml distilled or deionized water. Only use diluted WASHBUF when performing the assay. |
The diluted WASHBUF is stable up to one month at 4°C (2-8°C).
Standards & Controls for Serum, Plasma and Urine Measurements
|
1. |
Pipette 250 µl of distilled or deionized water into each standard (STD) and control (CTRL) vial. The exact concentration is printed on the label of each vial. |
|
2. |
Leave at room temperature (18-26°C) for 15 min. Vortex gently. |
Reconstituted STDs and CTRL are stable at -25°C or lower until expiry date stated on the label. Avoid freeze-thaw cycles!
Sample Preparation
Bring samples to room temperature and mix samples gently to ensure the samples are homogenous. We recommend duplicate measurements for all samples.
Samples for which the OD value exceeds the highest point of the standard range can be diluted with STD 1 or Big Endothelin-1 negative human serum.
Assay Protocol
Read the entire protocol before beginning the assay.
|
1. |
Bring reagents and samples to room temperature (18-24°C). |
|
2. |
Mark positions for STD/CTRL/SAMPLE (standard/control/sample) on the protocol sheet. |
|
3. |
Take microtiter strips out of the aluminum bag. Store unused strips with desiccant at 4°C in the aluminum bag. Strips are stable until expiry date stated on the label. |
|
4. |
Add 50 µl STD/CTRL/SAMPLE (standard/control/sample) in duplicates into the respective wells. |
|
5. |
Add 150 µl AB (biotinylated anti-Big Endothelin-1 antibody, green cap) into each well. Swirl gently. |
|
4. |
Cover the plate tightly, swirl gently and incubate for 4 hours at room temperature (18-24°C) in the dark. |
|
5. |
Aspirate and wash wells 5 x with 300 µl diluted WASHBUF. After the final wash, remove the remaining WASHBUF by strongly tapping plate against a paper towel. |
|
6. |
Add 200 µl CONJ (conjugate, amber cap) into each well. |
|
7. |
Cover tightly and incubate for 1 hour at room temperature in the dark. |
|
8. |
Aspirate and wash wells 5 x with 300 µl diluted WASHBUF. After the final wash, remove remaining WASHBUF by strongly tapping plate against a paper towel. |
|
9. |
Add 200 µl SUB (substrate, blue cap) into each well. |
|
10. |
Incubate for 30 min at room temperature in the dark. |
|
11. |
Add 50 µl STOP (stop solution, white cap) into each well. |
|
12. |
Measure absorbance immediately at 450 nm with reference 630 nm, if available. |
Calculation of Results
Read the optical density (OD) of all wells on a plate reader using 450 nm wavelength (reference wavelength 630 nm). If the OD of the highest STD is outside the measuring range of photometer the plate can be re-measured at 405 nm (correction wavelength 630 nm). Construct a standard curve from the absorbance read-outs of the standards using commercially available software capable of generating a four-parameter logistic (4-PL) fit. Alternatively, plot the standards’ concentration on the x-axis against the mean absorbance for each standard on the y-axis and draw a best fit curve through the points on the graph. Curve fitting algorithms other than 4-PL have not been validated and will need to be evaluated by the user.
Obtain sample concentrations from the standard curve. If required, pmol/l can be converted into pg/ml by applying a conversion factor (1 pg/ml =0.2335 pmol/l (MW: 4.283 kDa)). Respective dilution factors have to be considered when calculating the final concentration of the sample.
The quality control protocol supplied with the kit shows the results of the final release QC for each kit at production date. Data for OD obtained by customers may differ due to various influences and/or due to the normal decrease of signal intensity during shelf life. However, this does not affect validity of results as long as an OD of 1.00 or higher is obtained for the standard with the highest concentration and the control value is in range (target range see label).
INFORMATION ON THE ANALYTE
Big Endothelin-1 Protein
Big Endothelin-1 (BigET-1) is a peptide of 38 amino acids and is the precursor of Endothelin-1 (ET-1), consisting of amino acids 1-21 (http://www.uniprot.org/uniprot/P05305). ET-1 is a potent vasoconstrictor and is produced by vascular endothelial cells. Accordingly, it has a wide tissue distribution (http://www.ncbi.nlm.nih.gov/UniGene/ESTProfileViewer.cgi?uglist=Hs.511899). The cleavage of BigET-1 by Endothelin-converting enzyme (ECE) leads to Endothelin (ET) and to a C‑terminal fragment.
The half-life of ET-1 (1-21) in plasma is less than one minute, which may preclude its use as a diagnostic marker, whereas clearance of the precursor peptide BigET-1 is much slower. As Big-Endothelin-1 is produced at amounts equimolar to ET-1 and has higher plasma stability, it is more suitable for diagnostics and monitoring of heart failure (Gergei et al., 2018). Hence, Big ET-1 has the same physiological role as ET-1 while beeing a more reliable marker.
|
Molecular Weight |
4.283 kDa |
|
Cellular localisation |
Secreted |
|
Post-translational modifications |
Disulphide bonds, post-translational processing |
|
Sequence similarities |
Endothelin family |
|
Alternative Names |
For endothelin gene: Endothelin 1, Preproendothelin-1, Endothelin-1, PPET1, ARCND3, HDLCQ7, ET1, QME |
|
Entrez/NCBI ID |
|
|
Genecards |
EDN1: https://www.genecards.org/cgi-bin/carddisp.pl?gene=EDN1&keywords=edn1 |
|
OMIM |
131240: http://omim.org/entry/131240 |
|
PDB |
1T7H: http://www.rcsb.org/structure/1T7H ; |
|
Pfam |
Endothelin (PF00322): https://pfam.xfam.org/family/endothelin |
|
Protein Atlas |
EDN1 - https://www.proteinatlas.org/ENSG00000078401-EDN1/cell |
|
Uniprot ID |
EDN1 (P05305) - http://www.uniprot.org/uniprot/P05305 |
Big Endothelin-1 Function
Preproendothelin, a 203-amino-acid (AA) peptide is encoded by the ET-1 gene. It is converted into Big Endothelin-1 (Big ET-1), containing 38 amino acids. Big-ET-1 is then converted by the endothelin-converting enzyme (ECE) into the 21 AA biologically active Endothelin-1 peptide (AA1-21). Endothelin-1 circulates in low concentrations and has a very short plasma half-life. Big-Endothelin-1, the precursor is a stable peptide with a plasma half-life of about 30 minutes and measurement of Big ET-1 reflects Endothelin levels.
ET-1 is secreted, as a paracrine hormone, mainly from endothelial cells towards the smooth muscle cell layer of the vessels, to produce immediate vasoconstriction. Endothelin-1 (ET-1) has in fact been described as the most potent vasoconstrictor substance identified to date, and overactivation or dysfunction of the ET system has been implicated in the development and progression of hypertension in both clinical and experimental studies (Gillis EE et al., 2016). Big endothelin-1 has been demonstrated to be correlated with inflammation, endothelial dysfunction and arterial stiffness (Zhou BY et al., 2017). Both Big Endothelin and Endothelin are strong independent predictors of survival in patients with congestive heart failure and identify a population with very high-risk mortality. The pathophysiological roles of endothelin’s in the development of cardiovascular disease have been reviewed (Ohkita et al., 2012). It has been suggested that ET-1 is a major factor in the development of chronic kidney disease (CKD) as it contributes to hypertension, proteinuria, and renal inflammation in CKD. Numerous studies have demonstrated that ET-1 directly stimulates inflammation both in the vasculature and in the kidney, and this occurs in the absence of hypertension (Speed and Pollack, 2012).
Endothelins act via activation of two receptor subtypes, ETA and ETB receptors. Endothelin antagonists are currently used clinically in the treatment for patients with pulmonary hypertension (Davenport AP et al., 2016, Houde M et al., 2016), and are considered to have further target diseases as heart failure, cardiac hypertrophy and other cardiac diseases, renal diseases, systemic hypertension, and cerebral vasospasm (Miyauchi T and S Sakai, 2018).
-
Cancer
-
Oral squamous cell carcinoma (Mankapure et al., 2015)
-
Endothelin therapeutics in cancer (Rosanò and Bagnato, 2016)
-
-
Cardiology-Cardiovascular diseases
-
Prognostic value in heart failure and acute myocardial infarction (Gergei et al., 2017; Jankowich et al., 2016; Olivier et al., 2017)
-
Cardiomyopathy (Matsa et al., 2014; Yilu Wang et al., 2017)
-
Coronary artery disease and atherosclerosis (Chen et al., 2015; Qing et al., 2015; Wang et al., 2018; Yao Wang et al., 2017; Zhou et al., 2017)
-
Pulmonary hypertension (Yoshibayashi et al., 1991)
-
Pumonary thromboendarterectomy (Langer et al., 2005)
-
Cardiovascular disease (Ohkita et al., 2012)
-
Cardiovascular events (Jankowicha and Choudhary, 2019)
-
-
Nephrology
-
Renal insufficiency (Fischer et al.,2017)
-
During and after graft rejection (Jeremy et al., 2011)
-
Kidney disease and hypertension (Speed and Pollack, 2012)
-
-
Gillis et al., 2016 https://www.ncbi.nlm.nih.gov/pubmed/26936781
-
Zhou et al., 2017 - in Zotero, bereits unten angeführt
-
Ohkita et al., 2012 – in zotero
-
Speed and Pollack, 2012 , in Zotero
-
Fischer et al., 2017 https://www.ncbi.nlm.nih.gov/pubmed/28222015
-
Miyauchi and Sakai, 2018, https://www.ncbi.nlm.nih.gov/pubmed/30352269 (in Zotero angelegt, reviews - leider unter review im Endostatin ordner gerutscht, bitte ändern
-
Jankowicha and Choudhary, 2019 (in zotero angelegt) - leider unter review im Endostatin ordner gerutscht, bitte ändern
-
Yoshibayashi et al., 1991 https://www.ncbi.nlm.nih.gov/pubmed/1959183
-
Davenport et al., 2016, https://www.ncbi.nlm.nih.gov/pubmed/26956245
-
Houde et al., 2016, https://www.ncbi.nlm.nih.gov/pubmed/27451097
-
Langer et al., 2005 in zotero
-
Jeremy et al., 2011, in zotero angelegt. https://www.ncbi.nlm.nih.gov/pubmed/21056670
-
Rosanò and Bagnato, 2016- in zotero angelegt
All Biomedica ELISAs are validated according to FDA/ICH/EMEA guidelines. For more information about our validation guidelines, please refer to our quality page and published validation guidelines and literature.
Validation literature
1. ICH Q2(R1) Validation of Analytical Procedures: Text and Methodology.
2. EMEA/CHMP/EWP/192217/2009 Guideline on bioanalytical method validation.
3. Bioanalytical Method Validation, Guidance for Industry, FDA, May 2018
Calibration
This immunoassay is calibrated against recombinant human Big Endothelin-1 (1-38).
Detection Limit & Sensitivity
To determine the sensitivity of the Big Endothelin-1 ELISA, experiments measuring the lower limit of detection (LOD) and the lower limit of quantification (LLOQ) were conducted.
The LOD, also called the detection limit, is the lowest point at which a signal can be distinguished above the background signal, i.e. the signal that is measured in the absence of Big Endothelin-1, with a confidence level of 99%. It is defined as the mean back calculated concentration of standard 1 (0 pmol/l of Big Endothelin-1) plus three times the standard deviation of the measurements.
The LLOQ, or sensitivity of an assay, is the lowest concentration at which an analyte can be accurately quantified. The criteria for accurate quantification at the LLOQ are an analyte recovery between 75 and 125% and a coefficient of variation (CV) of less than 25%. To determine the LLOQ, standard 2, i.e. the lowest standards containing Big Endothelin-1, is diluted, measured and its concentration back calculated. The lowest dilution, which meets both criteria, is reported as the LLOQ.
The following values were determined for the Big Endothelin-1 ELISA:
|
LOD |
0.02 nmol/l |
|
LLOQ |
0.03 nmol/l |
Precision
The precision of an ELISA is defined as its ability to measure the same concentration consistently within the same experiments carried out by one operator (within-run precision or repeatability) and across several experiments using the same samples but conducted by several operators at different locations using different ELISA lots (in-between-run precision or reproducibility).
Within-Run Precision
Within-run precision was tested by measuring two samples 5 times within one human Big ET-1 ELISA lot. The experiment was conducted by one operator.
|
ID |
Within-Run Precision n |
Mean NT-proANP [pmol/l] |
SD [pmol/l] |
CV (%) |
|
Sample 1 |
5 |
0.20 |
0.003 |
2 |
|
Sample 2 |
5 |
1.00 |
0.048 |
5 |
In-Between-Run Precision
In-between-run precision was assessed by measuring two samples ten times within three human BigET-1 ELISA kit lots by three different operators.
|
ID |
In-Between Run Precision n |
Mean NT-proANP [pmol/l] |
SD [pmol/l] |
CV [%] |
|
Sample 1 |
10 |
0.20 |
0.009 |
4 |
|
Sample 2 |
10 |
1.0 |
0.041 |
4 |
Accuracy
The accuracy of an ELISA is defined as the precision with which it can recover samples of known concentrations.
The recovery of the Big Endothelin-1 ELISA was measured by adding recombinant Big Endothelin-1 to human samples containing a known concentration endogenous Big Endothelin-1. The %recovery of the spiked concentration was calculated as the percentage of measured compared over the expected value. All our ELISAs are expected to have %recovery rates within 15% of the nominal value of the sample.
This table shows the summary of the recovery experiments in the Big Endothelin-1 ELISA in different sample matrices:
|
% Recovery |
|||||
|
Sample Matrix |
n |
+ 1 pmol/l |
+ 2 pmol/l |
||
|
Mean |
Range |
Mean |
Range |
||
|
Serum |
14 |
100 |
80 - 127 |
105 |
85 – 119 |
|
EDTA plasma |
3 |
100 |
91 – 108 |
101 |
95 – 114 |
|
Citrate plasma |
3 |
98 |
83 -111 |
105 |
96 - 114 |
|
Heparin plasma |
3 |
97 |
92 – 108 |
102 |
96 – 109 |
Experiments:
Data showing recovery of recombinant Big Endothelin-1 in human serum samples:
|
Big Endothelin-1 [pmol/l] |
% Recovery |
||||||
|
Sample Matrix |
ID |
Reference |
+ 1 pmol/l |
+ 2 pmol/l |
+ 1 pmol/l |
+ 2 pmol/l |
|
|
Serum |
s1 |
0.65 |
1.6 |
2.7 |
97 |
102 |
|
|
Serum |
s2 |
0.8 |
2.1 |
2.9 |
117 |
104 |
|
|
Serum |
s3 |
0.02 |
1.3 |
2.4 |
127 |
119 |
|
|
Serum |
s4 |
0.3 |
1.5 |
2.4 |
115 |
104 |
|
|
Serum |
s5 |
0 |
1.1 |
2.5 |
110 |
125 |
|
|
Serum |
s6 |
0 |
0.9 |
2.2 |
90 |
110 |
|
|
Serum |
s7 |
0 |
1.0 |
2.3 |
100 |
115 |
|
|
Serum |
s8 |
0 |
0.8 |
1.7 |
80 |
85 |
|
|
Serum |
s9 |
0 |
0.8 |
1.9 |
80 |
95 |
|
|
Serum |
s10 |
0 |
1.1 |
1.9 |
110 |
95 |
|
|
Serum |
s11 |
0 |
1.0 |
2.1 |
100 |
105 |
|
|
Serum |
s12 |
0.1 |
1.1 |
2.3 |
100 |
110 |
|
|
Serum |
s13 |
0.06 |
0.9 |
1.8 |
85 |
87 |
|
|
Serum |
s14 |
0.06 |
0.9 |
2.3 |
85 |
112 |
|
|
Mean |
100 |
105 |
|||||
|
Min |
80 |
85 |
|||||
|
Max |
127 |
119 |
|||||
Data showing recovery of recombinant Big Endothelin-1 in human EDTA plasma samples:
|
Big Endothelin-1 [pmol/l] |
% Recovery |
||||||
|
Sample Matrix |
ID |
Reference |
+ 1 pmol/l |
+ 2 pmol/l |
+ 1 pmol/l |
+ 2 pmol/l |
|
|
EDTA plasma |
e1 |
0.11 |
1.2 |
2.4 |
108 |
114 |
|
|
EDTA plasma |
e2 |
0.09 |
1.1 |
2.1 |
101 |
100 |
|
|
EDTA plasma |
e3 |
0.1 |
1.0 |
2.0 |
91 |
95 |
|
|
Mean |
100 |
101 |
|||||
Data showing recovery of recombinant Big Endothelin-1 in a human citrate plasma sample:
|
Big Endothelin-1 [pmol/l] |
% Recovery |
||||||
|
Sample Matrix |
ID |
Reference |
+ 1 pmol/l |
+ 2 pmol/l |
+ 1 pmol/l |
+ 2 pmol/l |
|
|
Citrate plasma |
c1 |
0.11 |
1.1 |
2.4 |
99 |
114 |
|
|
Citrate plasma |
c2 |
0.08 |
1.2 |
2.2 |
111 |
106 |
|
|
Citrate plasma |
c3 |
0.08 |
0.9 |
2.0 |
83 |
96 |
|
|
Mean |
98 |
105 |
|||||
Data showing recovery of recombinant Big Endothelin-1 in a human heparin plasma sample:
|
Big Endothelin-1 [pmol/l] |
% Recovery |
||||||
|
Sample Matrix |
ID |
Reference |
+ 1 pmol/l |
+ 2 pmol/l |
+ 1 pmol/l |
+ 2 pmol/l |
|
|
Heparin plasma |
h1 |
0.11 |
1.2 |
2.3 |
108 |
109 |
|
|
Heparin plasma |
h2 |
0.09 |
1.0 |
2.0 |
92 |
96 |
|
|
Heparin plasma |
h3 |
0.08 |
1.0 |
2.1 |
93 |
101 |
|
|
Mean |
97 |
102 |
|||||
Dilution Linearity & Parallelism
Tests of dilution linearity and parallelism ensure that both endogenous and recombinant samples containing Big Endothelin-1 behave in a dose dependent manner and are not affected by matrix effects. Dilution linearity assesses the accuracy of measurements in diluted human samples spiked with known concentrations of recombinant analyte. By contrast, parallelism refers to dilution linearity in human samples and provides evidence that endogenous analyte behaves same way as the recombinant one. For dilution linearity and parallelism are assessed for each sample type and are considered good if the results are within 20% of the expected concentration.
Dilution linearity was assessed by serially diluting human samples spiked with 2 pmol/l recombinant Big Endothelin-1 with standard 1 (human serum containing 0 pmol/l Big Endothelin-1).
The table below show the mean recovery and range of serially diluted recombinant Big Endothelin-1 in serum:
|
% Recovery of recombinant Big Endothelin-1 in diluted samples |
|||||
|
Sample Matrix |
n |
1+1 |
1+3 |
||
|
Mean |
Range |
Mean |
Range |
||
|
Serum |
8 |
90 |
62- 105 |
96 |
71 - 126 |
Data showing dilution linearity of recombinant Big Endothelin-1 spiked into human blood samples (ref) containing endogenous Big Endothelin-1:
|
Big Endothelin-1 [pmol/l] |
% Recovery |
|||||
|
Sample Matrix |
ID |
Ref |
1+1 |
1+3 |
1+1 |
1+3 |
|
Serum |
s1 |
1.36 |
0.42 |
0.24 |
62 |
71 |
|
Serum |
s2 |
0.24 |
0.13 |
0.08 |
105 |
126 |
|
Serum |
s3 |
0.48 |
0.25 |
0.13 |
103 |
110 |
|
Serum |
s4 |
1.46 |
0.64 |
0.33 |
87 |
92 |
|
Serum |
s5 |
0.78 |
0.37 |
0.20 |
94 |
102 |
|
Serum |
s6 |
1.43 |
0.56 |
0.31 |
79 |
87 |
|
Serum |
s7 |
3.11 |
1.47 |
0.59 |
95 |
76 |
|
Serum |
s8 |
2.67 |
1.28 |
0.69 |
96 |
104 |
|
Mean |
90 |
96 |
||||
|
Min |
62 |
71 |
||||
|
Max |
105 |
126 |
||||
Parallelism was assessed by serially diluting human samples containing endogenous Big Endothelin-1 with with standard 1 (human serum containing 0 pmol/l Big Endothelin-1).
The table below show the mean recovery and range of serially diluted endogenous Big Endothelin-1 in several sample matrices:
|
% Recovery of endogenous Big Endothelin-1 in diluted samples |
|||||
|
Sample Matrix |
n |
1+1 |
1+3 |
||
|
Mean |
Range |
Mean |
Range |
||
|
EDTA plasma |
4 |
110 |
99 – 127 |
104 |
91 - 124 |
Data showing dilution linearity of endogenous Big Endothelin-1 in human EDTA plasma samples:
|
Big Endothelin-1 [pmol/l] |
% Recovery |
|||||
|
Sample Matrix |
ID |
Ref |
1+1 |
1+3 |
1+1 |
1+3 |
|
EDTA plasma |
e1 |
2.06 |
1.30 |
0.64 |
127 |
124 |
|
EDTA plasma |
e2 |
2.58 |
1.38 |
0.63 |
107 |
97 |
|
EDTA plasma |
e3 |
2.30 |
1.23 |
0.61 |
107 |
106 |
|
EDTA plasma |
e4 |
2.64 |
1.31 |
0.60 |
99 |
91 |
|
Mean |
110 |
104 |
||||
|
Min |
99 |
91 |
||||
|
Max |
127 |
124 |
||||
Specificity
This assay recognizes endogenous (natural) and recombinant human Big Endothelin-1 (Big ET-1).
Cross Reactivity
The factors listed below were assayed for cross-reactivity:
- Human ET1/2/3 (1-21): <1%
- Human ET2 (1-37): <1%
- Human ET1/2 (1-38): <1%
- Porcine BigET (1-39): 21%
- Human BigET1/2 (22-38): <1%
- Human BigET2 (22-37): <1%
- Rat BigET1 (1-39): 10%
- Sarafotoxin: <1%
Sample Stability
The stability of endogenous Big Endothelin-1 was tested by comparing Big Endothelin-1 measurements in samples that had undergone up to four freeze-thaw cycles.
For freeze-thaw experiments, samples were collected according to the supplier’s instruction using blood collection devices and stored at -80°C. Reference samples were freeze-thawed once. The mean recovery of sample concentration after four freeze-thaw cycles is 109%.
|
Big Endothelin-1 [pmol/l] |
% Recovery after 4 freeze/thaw cycles |
||||
|
ID |
1 x |
2 x |
3 x |
4 x |
|
|
s1 |
0.75 |
0.80 |
0.79 |
0.84 |
111 |
|
s2 |
0.15 |
0.14 |
0.12 |
0.17 |
120 |
|
s3 |
0.15 |
0.13 |
0.14 |
0.16 |
103 |
|
s4 |
0.84 |
0.79 |
0.86 |
0.84 |
100 |
|
Mean |
109 |
||||
Samples can undergo at least up to 3 freeze-thaw cycles.
Sample Values
To provide expected values for circulating Big Endothelin-1, a panel of samples from apparently healthy donors as well as samples from patient cohorts with cardiovascular and renal diseases were tested.
A summary of the results is shown below:
|
Big Endothelin-1 [pmol/l] |
|||||
|
Sample Matrix |
n |
Mean |
Median |
Minimum |
Maximum |
|
Apparently healthy |
41 |
0.22 |
0.09 |
0.01 |
1.58 |
|
Cardio panel |
30 |
0.8 |
0.6 |
0.2 |
2.1 |
|
Dialysis panel |
36 |
1.1 |
0.9 |
0.4 |
3.0 |
It is recommended to establish the normal range for each laboratory.
NT-proANP Values in an unselected hospital panel
NT-proANP was measured in patients from an unselected hospital panel. No medical histories were available.
|
Sample Matrix |
EDTA-plasma |
|
n |
40 |
|
Mean [nmol/l] |
3.89 |
|
Median [nmol/l] |
3.09 |
|
Min [nmol/l] |
0.63 |
|
Max [nmol/l] |
10.50 |
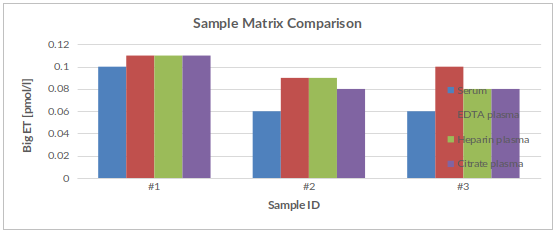
Matrix Comparision
To assess whether all tested matrices behave the same way in the Big Endothelin-1 ELISA, concentrations of Big Endothelin-1 were measured in serum, EDTA, heparin, and citrate plasma samples prepared from three apparently healthy donors. Each individual donated blood in all tested sample matrices.
A summary table of Big Endothelin-1 levels in various sample matrices is shown below:
|
Big Endothelin-1 [pmol/l] |
|||||
|
Sample ID |
Serum |
EDTA plasma |
Citrate plasma |
Heparin plasma |
% CV |
|
#1 |
0.1 |
0.11 |
0.11 |
0.11 |
7 |
|
#2 |
0.06 |
0.09 |
0.09 |
0.08 |
17 |
|
#3 |
0.06 |
0.1 |
0.08 |
0.08 |
23 |
A figure of Big Endothelin-1 levels in various sample matrices is shown below:
0:21 / 3:06
- The impact of antihypertensive pharmacotherapy on interplay between protein-bound uremic toxin (indoxyl sulfate) and markers of inflammation in patients with chronic kidney disease.
Kaminski, T.W., Pawlak, K., Karbowska, M., Znorko, B., Mor, A.L., Mysliwiec, M., Pawlak, D., 2019. Int Urol Nephrol.
- Novel approaches for the assessment of relative body weight and body fat in diagnosis and treatment of anorexia nervosa: A cross-sectional study.
Lackner, S., Mörkl, S., Müller, W., Fürhapter-Rieger, A., Oberascher, A., Lehofer, M., Bieberger, C., Wonisch, W., Amouzadeh-Ghadikolai, O., Moser, M., Mangge, H., Zelzer, S., Holasek, S.J., 2019. Human Nutrition.
- Is oxidized low-density lipoprotein the connection between atherosclerosis, cardiovascular risk and nephrolithiasis?
de Freitas, A.C.P., Torres, L.C., Duarte, M. do C.M.B., da Matta, M.C., Casarini, D.E., Schor, N., 2018. Urolithiasis.
 PMID:30302491
PMID:30302491 - Metabolic disorders and inflammation are associated with familial combined hyperlipemia.
Díaz-Ruiz, M., Martínez-Triguero, M.L., López-Ruiz, A., la Cruz, F.F., Bañuls, C., Hernández-Mijares, A., 2018. Clin. Chim. Acta.
PMID:30201373 - Bipolar disorder in youth is associated with increased levels of vitamin D-binding protein.
Petrov, B., Aldoori, A., James, C., Yang, K., Algorta, G.P., Lee, A., Zhang, L., Lin, T., Awadhi, R.A., Parquette, J.R., Samogyi, A., Arnold, L.E., Fristad, M.A., Gracious, B., Ziouzenkova, O., 2018. Transl Psychiatry 8, 61. PMCID: PMC5847532
PMID:29531242 - Whole-Body Cryotherapy Decreases the Levels of Inflammatory, Oxidative Stress, and Atherosclerosis Plaque Markers in Male Patients with Active-Phase Ankylosing Spondylitis in the Absence of Classical Cardiovascular Risk Factors.
Stanek, A., Cholewka, A., Wielkoszyński, T., Romuk, E., Sieroń, A., 2018. Mediators of Inflammation 2018, 1–11.
- Increased circulating oxidised low-density lipoprotein and antibodies to oxidised low-density lipoprotein in preeclampsia.
Arifin, R., Kyi, W.M., Che Yaakob, C.A., Yaacob, N.M., 2017. J Obstet Gynaecol 37, 580–584.
PMID:28358592 - Assessment of lipid profile and some risk factors of atherosclerosis in children whose parents had early onset coronary artery disease.
Bornaun, H., Öner, N., Nişli, K., Öztarhan, K., Yavuz, T., Türkoğlu, Ü., Dindar, A., Eker Ömeroglu, R., 2017a. Arch Argent Pediatr 115, 50–54.
PMID:28097840 - Evaluación del lipidograma y ciertos factores de riesgo de ateroesclerosis en niños cuyos padres tuvieron arteriopatía coronaria de inicio temprano.
Bornaun, H., Öner, N., Nişli, K., Öztarhan, K., Yavuz, T., Türkoğlu, Ü., Dindar, A., Eker Ömeroglu, R., 2017b. Archivos argentinos de pediatría 115, 50–57.
- Assessment of oxLDL, anti-oxLDL antibodies and lipoprotein-associated phospholipase A2 as cardiovascular risk markers in obese adolescents with and without T1DM.
Omar, N.N., EL Hefnawy, M.H., EL Soda, M.F., Heider, N.M., Hamed, H.I., 2017. Bulletin of Faculty of Pharmacy, Cairo University 55, 325–331.
- Cultivation and Immortalization of Human B-Cells Producing a Human Monoclonal IgM Antibody Binding to MDA-LDL: Further Evidence for Formation of Atherogenic MDA-LDL Adducts in Humans In Vivo.
Tatzber, F., Pursch, E., Resch, U., Pfragner, R., Holasek, S., Lindschinger, M., Cvirn, G., Wonisch, W., 2017. Oxidative Medicine and Cellular Longevity 2017, 1–7.
- DNA methylation patterns associated with oxidative stress in an ageing population.
Hedman, Å.K., Zilmer, M., Sundström, J., Lind, L., Ingelsson, E., 2016. BMC Medical Genomics 9, 72.
- Paraoxonase 1 activity and level of antibodies directed against oxidized low density lipoproteins in a group of an elderly population in Poland – PolSenior study.
Bednarska-Makaruk, M., Rodo, M., Szirkowiec, W., Mossakowska, M., Puzianowska-Kuźnicka, M., Skalska, A., Zdrojewski, T., Ryglewicz, D., Wehr, H., 2015. Archives of Gerontology and Geriatrics 60, 153–161.
- High reactive oxygen species in fibrotic and nonfibrotic skin of patients with diffuse cutaneous systemic sclerosis.
Bourji, K., Meyer, A., Chatelus, E., Pincemail, J., Pigatto, E., Defraigne, J.-O., Singh, F., Charlier, C., Geny, B., Gottenberg, J.-E., Punzi, L., Cozzi, F., Sibilia, J., 2015. Free Radic. Biol. Med. 87, 282–289.
PMID:26143738 - Metabolic and Inflammatory Profiles of Biomarkers in Obesity, Metabolic Syndrome, and Diabetes in a Mediterranean Population. DARIOS Inflammatory Study.
Fernández-Bergés, D., Consuegra-Sánchez, L., Peñafiel, J., Cabrera de León, A., Vila, J., Félix-Redondo, F.J., Segura-Fragoso, A., Lapetra, J., Guembe, M.J., Vega, T., Fitó, M., Elosua, R., Díaz, O., Marrugat, J., 2014. Revista Española de Cardiología (English Edition) 67, 624–631.
- Relationship of lipid oxidation with subhuman atherosclerosis and 10-year coronary events in general population.
Gómez, M., Vila, J., Elosua, R., Molina, L., Bruguera, J., Sala, J., Masià, R., Covas, M.I., Marrugat, J., Fitó, M., 2014. Atherosclerosis 232, 134–140.
PMID:24401227 - Effect of lifestyle changes and atorvastatin administration on dyslipidemia in hemodialysis patients: a prospective study.
Grzegorzewska, A.E., Niepolski, L., Sikora, J., Janków, M., Jagodziński, P.P., Sowińska, A., 2014. Polish Archives of Internal Medicine 124, 443–451.
- Analysis of 27 vascular-related proteins reveals that NT-proBNP is a potential biomarker for Alzheimer’s disease and mild cognitive impairment: A pilot-study.
Marksteiner, J., Imarhiagbe, D., Defrancesco, M., Deisenhammer, E.A., Kemmler, G., Humpel, C., 2014. Experimental Gerontology 50, 114–121.
- Anti-oxLDL antibodies are humanly insignificant for stroke patients.
Masztalewicz, M., Nowacki, P., Kotlęga, D., Bajer-Czajkowska, A., Drechsler, H., 2014. Neurol. Res. 36, 86–91.
PMID:24107551 - Antioxidant supplementation attenuates oxidative stress in patients undergoing coronary artery bypass graft surgery.
Stanger, O., Aigner, I., Schimetta, W., Wonisch, W., 2014. Tohoku J. Exp. Med. 232, 145–154
PMID:24573122 - Using Oxidized Low-Density Lipoprotein Autoantibodies to Predict Restenosis after Balloon Angioplasty in Patients with Acute Myocardial Infarction.
Huang, C.-H., Chang, C.-C., Huang, C.-S., Kuo, C.-L., Chen, C.-P., Hsia, C.-H., Chang, Y.-M., Chen, H.-T., Feng, C.-C., Lin, L.-S., Yang, P.-T., Tsai, C.-D., Lin, C.-S., Liu, C.-S., 2013. PLoS ONE 8, e74726.
- In depression, bacterial translocation may drive inflammatory responses, oxidative and nitrosative stress (O&NS), and autoimmune responses directed against O&NS-damaged neoepitopes.
Maes, M., Kubera, M., Leunis, J.-C., Berk, M., Geffard, M., Bosmans, E., 2013. Acta Psychiatr Scand 127, 344–354.
PMID:22900942 - Oxidative stress in post-acute ischemic stroke patients after intensive neurorehabilitation.
Ciancarelli, I., De Amicis, D., Di Massimo, C., Carolei, A., Ciancarelli, M.G.T., 2012. Curr Neurovasc Res 9, 266–273
PMID:22873723 - Imaging of inflamed carotid artery atherosclerotic plaques with the use of 99mTc-HYNIC-IL-2 scintigraphy in end-stage renal disease patients.
Opalinska, M., Stompor, T., Pach, D., Mikolajczak, R., Fedak, D., Krzanowski, M., Rakowski, T., Sowa-Staszczak, A., Glowa, B., Garnuszek, P., Maurin, M., Karczmarczyk, U., Sulowicz, W., Hubalewska-Dydejczyk, A., 2012. European Journal of Nuclear Medicine and Molecular Imaging 39, 673–682.
- Oxidized LDL to autoantibodies against oxLDL ratio – The new biomarker associated with carotid atherosclerosis and cardiovascular complications in dialyzed patients.
Pawlak, K., Mysliwiec, M., Pawlak, D., 2012. Atherosclerosis 224, 252–257.
- On the potential increase of the oxidative stress status in patients with abdominal aortic aneurysm.
Pincemail, J., Defraigne, J.O., Cheramy-Bien, J.P., Dardenne, N., Donneau, A.F., Albert, A., Labropoulos, N., Sakalihasan, N., 2012. Redox Rep. 17, 139–144.
PMID:22732574 - Functional muscle impairment in facioscapulohumeral muscular dystrophy is correlated with oxidative stress and mitochondrial dysfunction.
Turki, A., Hayot, M., Carnac, G., Pillard, F., Passerieux, E., Bommart, S., Raynaud de Mauverger, E., Hugon, G., Pincemail, J., Pietri, S., Lambert, K., Belayew, A., Vassetzky, Y., Juntas Morales, R., Mercier, J., Laoudj-Chenivesse, D., 2012. Free Radic. Biol. Med. 53, 1068–1079.
PMID:22796148 - Association between moderately oxidized low-density lipoprotein and high-density lipoprotein particle subclass distribution in hemodialyzed and post-renal transplant patients.
Kimak, E., Hałabiś, M., Baranowicz-Gąszczyk, I., Solski, J., Książek, A., 2011. Journal of Zhejiang University SCIENCE B 12, 365–371.
- Increased plasma peroxides as a marker of oxidative stress in myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS).
Maes, M., Kubera, M., Uytterhoeven, M., Vrydags, N., Bosmans, E., 2011. Med. Sci. Monit. 17, SC11-15 PMCID: PMC3539515
PMID:21455120 - Moderate consumption of red wine and human platelet responsiveness.
Tozzi Ciancarelli, M.G., Di Massimo, C., De Amicis, D., Ciancarelli, I., Carolei, A., 2011. Thromb. Res. 128, 124–129.
PMID:21489606 - Increased plasma peroxides and serum oxidized low density lipoprotein antibodies in major depression: markers that further explain the higher incidence of neurodegeneration and coronary artery disease.
Maes, M., Mihaylova, I., Kubera, M., Uytterhoeven, M., Vrydags, N., Bosmans, E., 2010. J Affect Disord 125, 287–294.
PMID:20083310 - Associations between Oxidized LDL to LDL Ratio, HDL and Vascular Calcification in the Feet of Hemodialysis Patients.
An, W.S., Kim, S.-E., Kim, K.-H., Bae, H.-R., Rha, S.-H., 2009. Journal of Korean Medical Science 24, S115.
- Effect of eicosapentaenoic and docosahexaenoic acid on resting and exercise-induced inflammatory and oxidative stress biomarkers: a randomized, placebo controlled, cross-over study.
Effect of eicosapentaenoic and docosahexaenoic acid on resting and exercise-induced inflammatory and oxidative stress biomarkers: a randomized, placebo controlled, cross-over study.
- Grape extract improves antioxidant status and physical performance in elite male athletes.
Lafay, S., Jan, C., Nardon, K., Lemaire, B., Ibarra, A., Roller, M., Houvenaeghel, M., Juhel, C., Cara, L., 2009 13
- Oxidized LDL and anti‐oxLDL antibody levels in peripheral atherosclerotic disease.
Andican, G., Seven, A., Uncu, M., Cantaşdemir, M., Numan, F., Burçak, G., 2008. Scandinavian Journal of Human and Laboratory Investigation 68, 473–478.
- Perceived work-related stress and early atherosclerotic changes in healthy employees.
Bugajska, J., Widerszal-Bazyl, M., Radkiewicz, P., Pasierski, T., Szulczyk, G.A., Ząbek, J., Wojciechowska, B., Jędryka-Góral, A., 2008. International Archives of Occupational and Environmental Health 81, 1037–1043.
- Effect of different contraceptive methods on the oxidative stress status in women aged 40 48 years from the ELAN study in the province of Liege, Belgium.
Pincemail, J., Vanbelle, S., Gaspard, U., Collette, G., Haleng, J., Cheramy-Bien, J.P., Charlier, C., Chapelle, J.P., Giet, D., Albert, A., Limet, R., Defraigne, J.O., 2007. Hum. Reprod. 22, 2335–2343.
PMID:17584753 - Effects of reconstituted HDL on charge-based LDL subfractions as characterized by capillary isotachophoresis.
Zhang, B., Uehara, Y., Hida, S., Miura, S., Rainwater, D.L., Segawa, M., Kumagai, K., Rye, K.-A., Saku, K., 2007. J. Lipid Res. 48, 1175–1189.
PMID:17327623 - Relationship of classical and non-classical risk factors with genetic variants relevant to coronary heart disease.
Manresa, J.M., Zamora, A., Tomás, M., Sentí, M., Fitó, M., Covas, M.I., Alcántara, M., Latorre, G., Escurriol, V., Domingues, S., Marrugat, J., 2006. Eur J Cardiovasc Prev Rehabil 13, 738–744.
PMID:17001213 - Reduction of oxidative stress and modulation of autoantibodies against modified low-density lipoprotein after rosuvastatin therapy.
Resch, U., Tatzber, F., Budinsky, A., Sinzinger, H., 2006. Br J Clin Pharmacol 61, 262–274. PMCID: PMC1885020
PMID:16487219 - Circulating oxidized low density lipoprotein, autoantibodies against them and homocysteine serum levels in diagnosis and estimation of severity of coronary artery disease.
Faviou, E., Vourli, G., Nounopoulos, C., Zachari, A., Dionyssiou-Asteriou, A., 2005. Free Radic. Res. 39, 419–429
PMID:16028367 - Evaluation of autoantibodies against oxidized LDL (oLAB) and blood antioxidant status in professional soccer players.
Kłapcińska, B., Kempa, K., Sobczak, A., Sadowska-Krepa, E., Jagsz, S., Szołtysek, I., 2005. Int J Sports Med 26, 71–78.
PMID:15643538 - Alteration of the Copy Number of Mitochondrial DNA in Leukocytes of Patients with Hyperlipidemia.
Liu, C.-S., Kuo, C.-L., Cheng, W.-L., Huang, C.-S., Lee, C.-F., Wei, Y.-H., 2005. Annals of the New York Academy of Sciences 1042, 70–75.
- Autoantibodies against oxidized low-density lipoprotein (ox-LDL) and LDL oxidation status.
Brizzi, P., Tonolo, G., Bertrand, G., Carusillo, F., Severino, C., Maioli, M., Malaguarnera, L., Musumeci, S., 2004. Clin. Chem. Lab. Med. 42, 164–170.
PMID:15061355 - The 161TT genotype in the exon 6 of the peroxisome-proliferator-activated receptor γ gene is associated with premature acute myocardial infarction and increased lipid peroxidation in habitual heavy smokers.
Chao, T.-H., Li, Y.-H., Chen, J.-H., Wu, H.-L., Shi, G.-Y., Liu, P.-Y., Tsai, W.-C., Guo, H.-R., 2004. Human Science 107, 461–466.
PMID:15217350 - Antibodies to oxidized low-density lipoprotein in patients following coronary artery revascularization.
Miller, E.R., Erlinger, T.P., Blumenthal, R.S., Margolis, S., Allen, J.K., 2003. Coron. Artery Dis. 14, 163–169.
PMID:12655280 - Antibodies against ox-LDL serum levels in patients with hepatocellular carcinoma.
Motta, M., Pistone, G., Franzone, A.M., Romeo, M.A., Di Mauro, S., Giugno, I., Ruello, P., Malaguarnera, M., 2003. Panminerva Med 45, 69–73
PMID:12682623 - The association of antibodies against oxidized low-density lipoprotein with atherosclerosis in hemodialysis patients.
Shoji, T., Kimoto, E., Shinohara, K., Emoto, M., Ishimura, E., Miki, T., Tsujimoto, Y., Tabata, T., Nishizawa, Y., 2003. Kidney Int. Suppl. S128-130.
PMID:12694327 - Evaluation of the atherogenic tendency of lipids and lipoprotein content and their relationships with oxidant-antioxidant system in patients with psoriasis.
Vanizor Kural, B., Orem, A., Cimşit, G., Yandi, Y.E., Calapoglu, M., 2003. Clin. Chim. Acta 328, 71–82
PMID:12559600 - Oral L-arginine does not improve endothelial dysfunction in children with chronic renal failure.
Bennett-Richards, K.J., Kattenhorn, M., Donald, A.E., Oakley, G.R., Varghese, Z., Bruckdorfer, K.R., Deanfield, J.E., Rees, L., 2002. Kidney Int. 62, 1372–1378.
PMID:12234308 - Antibody to oxidized low-density lipoprotein and cardiovascular mortality in end-stage renal disease.
Shoji, T., Fukumoto, M., Kimoto, E., Shinohara, K., Emoto, M., Tahara, H., Koyama, H., Ishimura, E., Nakatani, T., Miki, T., Tsujimoto, Y., Tabata, T., Nishizawa, Y., 2002. Kidney Int. 62, 2230–2237.
PMID:12427150 - Decreased oxidative stress in patients with idiopathic dilated cardiomyopathy one year after immunoglobulin adsorption.
Schimke, I., Müller, J., Priem, F., Kruse, I., Schön, B., Stein, J., Kunze, R., Wallukat, G., Hetzer, R., 2001. Journal of the American College of Cardiology 38, 178–183.
- Acute and long-term effects of low-density lipoprotein (LDL)-apheresis on oxidative damage to LDL and reducing capacity of erythrocytes in patients with severe familial hypercholesterolaemia.
Stefanutti, C., Giacomo, S.D., Vivenzio, A., Isacchi, G.C., Masella, R., Caprari, P., Varì, R., Tarzia, A., Mosiello, A., Cantafora, A., 2001. Human Science 100, 191–198.
PMID:11171288 - Inverse relationship between circulating oxidized low density lipoprotein (oxLDL) and anti-oxLDL antibody levels in healthy subjects.
Shoji, T., Nishizawa, Y., Fukumoto, M., Shimamura, K., Kimura, J., Kanda, H., Emoto, M., Kawagishi, T., Morii, H., 2000. Atherosclerosis 148, 171–177.
- Strong association between malnutrition, inflammation, and atherosclerosis in chronic renal failure.
Stenvinkel, P., Heimbürger, O., Paultre, F., Diczfalusy, U., Wang, T., Berglund, L., Jogestrand, T., 1999. Kidney Int. 55, 1899–1911.
PMID:10231453 - Autoantibodies against oxidated low density lipoproteins (oLAb) and procalcitonin (PCT) as prognostic markers for patients suffering from sepsis and systemic inflammatory response syndrome (SIRS).
Reiger, J., Tatzber, F., Ziervogel, G., Köller, U., Grimm, G., 1998. Crit Care 2, P006. PMCID: PMC3301248
- Lipid peroxidation parameters and antioxidant status of critically ill intensive care unit patients.
Smolle, K., Khoschsorur, G., Wonisch, W., Tatzber, F., 1998. Crit Care 2, P012. PMCID: PMC3301254
